How can Deep Breathing be beneficial for our health
Breathing is an essential element of our existence and biological activities. In this review we are looking at the benefits of deep breathing during physical activities and its effect on cardiovascular system (CVS) (1). The rate of respiration and the volume of air inhale can be voluntary as well as involuntary and it is controlled by cranial (CN IX and CN X) and spinal (C3, 4 and 5) nerves 2. CN IX and CN X directly influence the heart and its blood vessels and in turn regulate respiration by gas exchange between haemoglobin of the red blood cells and endothelial cell of the alveoli (2).
Therefore blood is a contributing factor that influences breathing as it supplies oxygen to the haemoglobin of the red blood cells. This could be the reason for higher value of red blood cells in people living at higher altitude, as there is less oxygen in the air (3).
It has been shown that high altitude reduces the volume and function of mitochondria 4, indicating that O2 regulates mitochondrial function 5. Thus deep breathing exercise adjusts the partial pressures of O2(PO2) and CO2(PCO2) and regulates conditions such as hypertension and hypotension, and related cardiovascular diseases 6,7. These pathological conditions could be due to the dysfunction of mitochondria and resultant increase in production of Reactive Oxygen Species (ROS) (5).
Literature clearly appreciates the influence of the respiratory system in the modifications of cardiovascular system’s performance (8) due to the regular exercise (2). In Early 90’s, scientists exhibited the effect and benefits of meditation on enhancing positive mental power and subsequent reduction in anxiety and illicit drug consumption (9).
Transcendental Meditation begins with synchronised deep breathing and is the first physiological modification for improving our health. Cardiovascular disease, stress and anxiety are interrelated and
mindfulness treatment shows significant positive results (10).
They are a direct relationship between deep breathing and efficient gas exchange, which is essential for the development of capillary networks in muscle and lungs. These alterations in angiogenesis, which is the development of the capillary network, are synchronised with the cardiovascular system (11). There is an immediate effect of deep breathing exercises on atelectasis and oxygenation of heart, lungs and muscles (12).
Literature indicated that deep-breathing exercise reduces atelectasis and improves pulmonary function after coronary artery bypass surgery (13).

What is Deep Breathing?
Deep Breathing is a relaxation technique where the focus is on deep inhalation, and holding the breath for a few seconds before exhalation (14). It is uncommonly used by few psychologists for patients suffering from psychological disorders (14). Research exhibits the effect of mindfulness and stress reduction such as for the treatment of anxiety disorder (15).
However, there is an interest in developing this technique for rehabilitation therapies 16, which has been used for centuries in Asia under different forms of practice such as Tai Chi, Qi Gong, Yoga and meditation (1, 14, 17-20). In deep breathing the main biological structures are diaphragm, pleural membrane and the alveoli; any modification in the exchange of gases and nutrients in the blood capillaries is conducted by the heart and lungs (21).
Diffusion of the gases are not only directly related to the atmospheric and PO2 and carbon dioxide PCO2 but also to the surface area of the capillaries and alveoli (22). Therefore, deep breathing will not only enhance the efficiency of the lungs for the gas exchange2 but also positively regulate and sustain the function of the cardiovascular system (14, 16, 23).
Warm Up and Deep Breathing During Health and Disease
Deep breathing becomes a very important factor for physical activities in relation to cardiovascular changes such as increase in cardiac output which in turn increases the blood flow in capillaries and muscles (24). A warm up exercise not only increases the electro-stimuli of cardiovascular and cerebrovascular systems but also results in the flexibility of the joints along with an increase in the breathing rate (25).
Similarly, deep breathing exercises with positive expiratory pressure at a higher rate improve oxygenation (26) and in conditions such as recovering from a trauma or during rehabilitation, the deep breathing exercises including Qi Gong, Tai Chi, Yoga and meditation improves physical and mental strength (17-20).
Activities in Qi Gong or Tai Chi are usually combined with regular and synchronised breathing that allows a higher volume of O2 uptake (27) and all muscles in the body including heart muscles learn to contract and relax at a specific body position during these exercises (28). Similarly Yoga and meditation allow breathing improvement and reduce the sensitivity of chemo and cardio reflex due to a reduction of the breathing and heart rate (20).
Deep breathing techniques increase the efficacy of pre oxygenation and hence rises the tidal volume (29,30). Similarly, a short term training of yoga for the patients of Chronic Obstructive Pulmonary Disease (COPD) induces favourable changes in the respiratory and cardiovascular system (1).
The Physiology of Respiratory and Cardiovascular Interaction
Neuronal interaction and control
Both Phrenic (C3 to C5) and Vagus (CN10) nerves not only interact with each other (31) but are associated with the direct control of respiratory and cardiovascular systems (32). Intercostal and diaphragm muscles are regulated via phrenic nerves (C3, C4 and C5), which is responsible for the decrease in partial pressure of the lungs by increasing their volume (2). Similarly, stretch receptors in the lungs allow vagal afferent pathways to moderate inflation (33) and modulate the heart rate, through autonomic nervous system (34). The vagus nerve, which originates from the nucleus ambiguous, is not only associated with the breathing process but also controls cardiac function (35). The pontine respiratory group, also known as pneumotaxic centre has an inhibitory effect on inhalation through the dorsal respiratory group (DRG), whereas, the apneustic center has a stimulating effect on DRG to promote inhalation (36). Similarly, ventral respiratory group (VRG) in conjunction with DRG regulate the respiratory rate (37), also controlled by glossopharyngeal nerve (cranial nerve IX) (38). This nerve is also involved in controlling the heart velocity (39), which is regulated by cardiac baroreflex, blood pressure and O2 concentration (40). The heart rate is regulated by sympathetic and parasympathetic neurons via afferent vagal pathway (41), similarly, the aortic and carotid baroreflexes are associated with breathing (42) and hypotension (43).
(Refer to Figure 1 below.)
Regulation of Lungs, Heart and Blood Vessels by Peripheral Nervous System
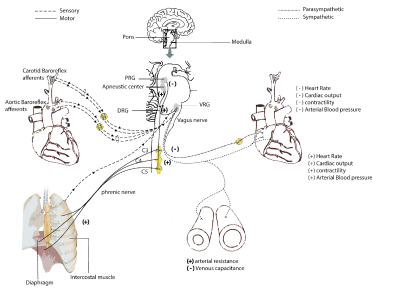
Figure 1: Showing the locations of pons and medulla in the brain stem with Pontine Respiratory Group (PRG) or Pneumotaxic centre, the Apneustic centre, Dorsal Respiratory Group (DRG) and Ventral Respiratory Group (VRG). The interaction between the sensory signals of the carotid and aortic baroreflex as well as the stretch receptor in the airways and the motor signals that activate the diaphragm and the intercostal muscle
are shown in this figure. Also the interaction between sympathetic and parasympathetic signals on lungs, heart and blood vessels is depicted. It displays sensory and motor nerves (left) and parasympathetic and sympathetic pathways (right). The Vagus nerve innervates the heart and blood vessels on the right side of the diagram. Phrenic nerve innervates lungs and diaphragm on the left side of the diagram. Tortora Gerard, inspired this diagram from Principles of anatomy and physiology the 12th edition published in 2008 (44).
Regulation of Breathing and Heart Rate
All components of the respiratory system including nose, pharynx, larynx, trachea, bronchi, bronchioles and alveoli are not only important for speech, warming, humidifying and filtering the air and gas exchange (45) but are also involved in the regulation of the cardiovascular system during deep breathing exercise (46). During this exercise, the decrease in inhalation/exhalation ratio allows the heart to slow down, the diaphragm to relax and the lungs to inflate and deflate with greater efficiency (47). Consequently, deep breathing increases the pressure and the flow of air from inside to outside of lungs (2). This difference in pressure allows an increase in gas exchange between the lungs and the capillaries, which is detected by the baroreceptors present in the aortic and carotid arteries (40) and lungs (48).
The chemoreceptors present at the medulla and pons detect the O2 / CO2 ratio and pH (49) and regulate the breathing and heart rate through the vagus nerve (50). Inhibition or stimulation of the vagus nerve is directly related with the modification of blood pressure, heart rate and breathing rate50 and deep breathing exercises bring these values back to normal (51). Both inspiratory and expiratory centres are located in medulla and pons (52).
Stimulation of the inspiratory centres that are located at the dorsal part of the medulla (53) and pons, results in the expansion of the intercostal muscles, diaphragm and the lungs, decreasing the internal pressure and allowing the air to go inside the body. On the other hand, the expiratory centres which are present at the ventral side of the medulla (54), and pneumotaxic centres that are located at the upper parts of the pons are responsible for controlling the rate and pattern of breathing, and are regulated by the apneustic centres (55). The apneustic centre enhances inspiration and the stimulation of the pneumotaxic centre and the stretch receptors of the lungs resulting in exhalation and diaphragm relaxation (36). The receptors on the pons and medulla that are sensitive to pH fluctuation activates the locus coeruleus or nucleus ambiguous that increases or decreases heart rate and breathing to bring the pH back to normal (56). The vagus innervation from the enteric nervous system also has a significant role in the regulation of cardiovascular and respiratory systems and is influenced by the receptors on the carotid arteries and brain stem (57). The vagus nerve which contains both motor and sensory inputs spread throughout the brachial and visceral areas (58) inducing parasympathetic control. This mechanism has a direct effect on blood pressure, heart and muscles (Fig 1). On the other hand, the sympathetic response has the opposite effect (59) and arterial pressure can act as a biomarker (60).
In addition, different positions of the body can affect the flow of blood and therefore modify the gas exchange (2). The positions during standing or sitting changes the respiratory parameters, for example in the sitting position the vital capacity (VC), forced vital capacity (FVC), forced expiratory volume in the first second (FEV1) and the peak expiratory flow (PEF) are reduced (61).
The Benefits of Deep Breathing
Though all the cell organelles are affected by the gas exchange, the mitochondria plays an essential role in the conversion of oxygen into Adenosine Triphosphate (ATP) (62). Mitochondrial dysfunction is directly related to hypertension, cardiovascular and circulatory disorders such as stroke, diabetes, Alzheimer’s disease and Parkinson disease (63-65). It is well known that physical exercise has a positive effect on the cardiovascular system and on cognition (66) and deep breathing alleviate stress anxiety and depression (67).
Similarly, social threats such as public speech and participating in sports events can alter the cardiovascular system (68) and deep breathing can result in improved performance (47). In a study, it was shown that exercise 3 to 5 times per week at moderate intensity reduces the blood pressure (69). The study showed significant decrease in systolic blood pressure of both hypertensive and normotensive subjects; whereas, only diastolic blood pressure was found to decrease in hypertensive subjects (7, 69).
Literature shows that during exercise the increased blood pressure delivers more nutrients and oxygen to the body and removes waste from the tissues through the circulatory system (2, 70). On the other hand, it was revealed that the risk of stroke increases during intense exercise when systolic blood pressure rises more than 19.7 mmHg per minute (70). For that reason, it is fundamental to learn breathing techniques, such as Pranayama, when practising sport activities any form of mindfulness (71). The principle of pranayama breathing is based on a longer exhalation than inhalation (14) which decreases the rate of gas exchange. The literature indicates that pranayama breathing also decreases heart rate, O2 consumption, and blood pressure (14,34,72). It has also been revealed that the pranayama breathing technique allows parasympathetic dominance (14,73), hence enhancing a relaxation state. Therefore the electro activity diminished allowing muscle fibers to relax longer before the next action potential (72). This electrical shift was measured using Respiratory Sinus Arrhythmia (RSA), Electrocardiogram (ECG) and Electroencephalogram (EEG) (74).
One of the major benefits of deep breathing techniques is to increase the gas exchange process, due to the development of the capillary network by the release of cytokines for angiogenesis (75). Angiogenesis takes place by different processes such as intussusception, which is the blood vessel that splits and grows, or the sprouting of blood vessels which is more for proliferation and development (11). During muscle contraction more blood vessels are required for appropriate gas exchange (76). In a study, it was reported that nitric oxide is the leading compound to generate vessel growth during exercise (76). The intussusceptive angiogenesis results in the enlargement of vessels, which in turn increases blood volume and gas exchange (76,77). There is no evidence to date that angiogenesis is occurring in the lungs during exercise. However, in lungs angiogenesis may occur due to the friction caused by the constant blood flow in vessels, releasing nitric oxide from their endothelium (5).
To conclude, The vagus nerves, originating from the nucleus ambiguous, have both sympathetic and parasympathetic effect on the circulatory system (78,79). A sympathetic response increases the heart rate, cardiac output; contractility and arterial blood pressure; whereas the parasympathetic response has the opposite effect (2, 44). Deep breathing increases the amount of gas exchange (80) and allows nutrients and O2 to increase the amount of ATP production in the mitochondria and rebalance the pH of the body due to the change in cardiac output (81).
This mechanism gives energy to the cell and produces waste material (2). Evidence is required to confirm the process of angiogenesis in the lungs. Breathing affects multiple metabolic processes such as the conversion of inactive angiotensin I from the liver into angiotensin II which affect the cardiovascular system (82, 83). Respiration also plays an important role in the breakdown of substances such as noradrenaline, serotonin and acetylcholine (45, 84, 85) which are regulators of moods and behaviours. This review develops possible research and theoretical knowledge on the effect of activities such as Tai Chi, Qi Gong, Yoga and meditation on respiratory and cardiovascular systems (1,17,18,46). And more importantly, it opens the discussion on possible non-invasive therapies where patients are also prescribed activities for a better rehabilitation (86, 87).
Reference:
1. Mamtani R, Mamtani R. Ayurveda and yoga in cardiovascular diseases. Cardiology in review. 2005;13(3):155-162.
2. McArdle WD, Katch FI, Katch VL. Exercise Physiology: Nutrition, Energy, and Human Performance. Wolters Kluwer - Lippincott Williams & Wilkins; 2014. 3. Grover RF, Weil JV, Reeves JT. Cardiovascular adaptation to exercise at high altitude. Exercise and sport sciences reviews. 1986;14:269-302.
4. Murray AJ, Horscroft JA. Mitochondrial function at extreme high altitude. The Journal of physiology. 2016;594(5):1137-1149.
5. Ballinger SW. Mitochondrial dysfunction in cardiovascular disease. Free Radical Biology and Medicine. 2005;38(10):1278-1295.
6. Gardner WN. The pattern of breathing following step changes of alveolar partial pressures of carbon dioxide and oxygen in man. The Journal of
Physiology. 1980;300(1):55-73.
7. Paul G, Elam B, Verhulst SJ. A longitudinal study of students' perceptions of using deep breathing meditation to reduce testing stresses. Teaching and
learning in medicine. 2007;19(3):287-292.
8. Joyner MJ, Green DJ. Exercise protects the cardiovascular system: effects beyond traditional risk factors. The Journal of physiology.
2009;587(23):5551-5558.
9. Alexander CN, Robinson P, Orme-Johnson DW, Schneider RH. The effects of transcendental meditation compared to other methods of relaxation and
meditation in reducing risk factors, morbidity, and mortality. Homeostasis in Health and Disease. 1994.
10. Tacón AM, McComb J, Caldera Y, Randolph P. Mindfulness meditation, anxiety reduction, and heart disease: a pilot study. Family & community health.
2003;26(1):25-33.
11. Djonov V, Baum O, Burri PH. Vascular remodeling by intussusceptive angiogenesis. Cell and tissue research. 2003;314(1):107-117.
12. Westerdahl E, Lindmark B, Eriksson T, Hedenstierna G, Tenling A. The immediate effects of deep breathing exercises on atelectasis and oxygenation after cardiac surgery. Scandinavian Cardiovascular Journal.
2003;37(6):363-367.
13. Westerdahl E, Lindmark B, Eriksson T, Hedenstierna G, Tenling A. Deep-breathing exercises reduce atelectasis and improve pulmonary function after coronary artery bypass surgery. Chest. 2005;128(5):3482-3488.
14. Jerath R, Edry JW, Barnes VA, Jerath V. Physiology of long pranayamic breathing: neural respiratory elements may provide a mechanism that explains how slow deep breathing shifts the autonomic nervous system. Medical hypotheses. 2006;67(3):566-571.
15. Miller J, Fletcher K, Kabat-Zinn J. Three-year follow-up and clinical implications of a mindfulness meditation-based stress reduction intervention in the treatment of anxiety disorders. International Journal of Yoga Therapy. 1998;8(1):45-53.
16. Celli BR, Rodriguez KS, Snider GL. A Controlled Trial of Intermittent Positive Pressure Breathing, Incentive Spirometry, and Deep Breathing Exercises in Preventing Pulmonary Complications after Abdominal Surgery 1–4. American Review of Respiratory Disease. 1984;130(1):12-15.
17. Wang C, Collet JP, Lau J. The effect of Tai Chi on health outcomes in patients with chronic conditions: a systematic review. Archives of internal medicine. 2004;164(5):493-501.
18. Wall RB. Tai chi and mindfulness-based stress reduction in a Boston public middle school. Journal of Pediatric Health Care. 2005;19(4):230-237. 19. Gilbert C. Yoga and breathing. Journal of Bodywork and movement therapies. 1999;3(1):44-54.
20. Spicuzza L, Gabutti A, Porta C, Montano N, Bernardi L. Yoga and chemoreflex response to hypoxia and hypercapnia. The Lancet.
2000;356(9240):1495-1496.
21. Kawakami Y, Natelson BH, DuBois AR. Cardiovascular effects of face immersion and factors affecting diving reflex in man. Journal of Applied Physiology. 1967;23(6):964-970.
22. Jensen FB. Red blood cell pH, the Bohr effect, and other oxygenation‐linked phenomena in blood O2 and CO2 transport. Acta Physiologica.
2004;182(3):215-227.
23. Jerath R, Barnes VA. Augmentation of mind-body therapy and role of deep slow breathing. Journal of Complementary and Integrative medicine. 2009;6(1).
24. Araújo CGS, Nóbrega ACL, Castro CLB. Heart rate responses to deep breathing and 4-seconds of exercise before and after pharmacological blockade with atropine and propranolol. Clinical autonomic research. 1992;2(1):35-40.
25. Warnke U. Electromagnetic sensitivity of animals and humans: Biological and clinical implications. Bioelectrodynamics and Biocommunication: World Scientific; 1994:365-386.
26. Urell C, Emtner M, Hedenström H, Tenling A, Breidenskog M, Westerdahl E. Deep breathing exercises with positive expiratory pressure at a higher rate improve oxygenation in the early period after cardiac surgery—a randomised controlled trial. European Journal of Cardio-thoracic Surgery.
2011;40(1):162-167.
27. Lan C, Lai J-S, Wong M-K, Yu M-L. Cardiorespiratory function, flexibility, and body composition among geriatric Tai Chi Chuan practitioners. Archives of physical medicine and rehabilitation. 1996;77(6):612-616.
28. Song R, Lee E-O, Lam P, Bae S-C. Effects of tai chi exercise on pain, balance, muscle strength, and perceived difficulties in physical functioning in older women with osteoarthritis: a randomized clinical trial. The Journal of Rheumatology. 2003;30(9):2039-2044.
29. Nimmagadda U, Salem MR, Joseph NJ, Miko I. Efficacy of preoxygenation using tidal volume and deep breathing techniques with and without prior maximal exhalation. Canadian Journal of Anesthesia. 2007;54(6):448-452.
30. Nimmagadda U, Chiravuri SD, Salem MR, et al. Preoxygenation with tidal volume and deep breathing techniques: the impact of duration of breathing and fresh gas flow. Anesthesia & Analgesia. 2001;92(5):1337-1341.
31. Paton JFR, Boscan P, Pickering AE, Nalivaiko E. The yin and yang of cardiac autonomic control: vago-sympathetic interactions revisited. Brain Research Reviews. 2005;49(3):555-565.
32. Bartoli A, Cross BA, Guz A, Huszczuk A, Jefferies R. The effect of varying tidal volume on the associated phrenic motoneurone output: studies of vagal and chemical feedback. Respiration physiology. 1975;25(2):135-155.
33. Schelegle ES. Functional morphology and physiology of slowly adapting pulmonary stretch receptors. The anatomical record. 2003;270(1):11-16. 34. Pal GK, Velkumary S. Effect of short-term practice of breathing exercises on autonomic functions in normal human volunteers. Indian Journal of Medical Research. 2004;120(2):115.
35. Wang J, Irnaten M, Neff RA, et al. Synaptic and neurotransmitter activation of cardiac vagal neurons in the nucleus ambiguus. Annals of the New York Academy of Sciences. 2001;940(1):237-246.
36. Plum F. Neural mechanisms of abnormal respiration in humans. Archives of neurology. 1960;3(5):484-487.
37. Smith JC, Ellenberger HH, Ballanyi K, Richter DW, Feldman JL. Pre-Bötzinger complex: a brainstem region that may generate respiratory rhythm in mammals. Science (New York, NY). 1991;254(5032):726.
38. Duffin J, Ezure K, Lipski J. Breathing rhythm generation: focus on the rostral ventrolateral medulla. Physiology. 1995;10(3):133-140.
39. Hosseini SM, Jamshir M, Maleki A. The effect of gag reflex on cardiac sympatovagal tone. Oman medical journal. 2012;27(3):249.
40. Heistad D, Abboud FM, Mark AL, Schmid PG. Effect of baroreceptor activity on ventilatory response to chemoreceptor stimulation. Journal of Applied Physiology. 1975;39(3):411-416.
41. Swenne CA. Baroreflex sensitivity: mechanisms and measurement. Netherlands Heart Journal. 2013;21(2):58-60.
42. Brunner MJ, Sussman MS, Greene AS, Kallman CH, Shoukas AA. Carotid sinus baroreceptor reflex control of respiration. Circulation Research.
1982;51(5):624-636.
43. Sanders JS, Mark AL, Ferguson DW. Importance of aortic baroreflex in regulation of sympathetic responses during hypotension. Evidence from direct sympathetic nerve recordings in humans. Circulation. 1989;79(1):83-92.
44. Tortora GJ, Nielsen M. Principles of Human Anatomy. Wiley Global Education; 2016.
45. Ward J. Physiology of breathing I. Surgery (Oxford). 2005;23(11):419-424.
46. Vyas R, Dikshit N. Effect of meditation on respiratory system, cardiovascular system and lipid profile. Indian journal of physiology and pharmacology. 2002;46(4):487-491.
47. Van Diest I, Verstappen K, Aubert AE, Widjaja D, Vansteenwegen D, Vlemincx E. Inhalation/exhalation ratio modulates the effect of slow breathing on heart rate variability and relaxation. Applied psychophysiology and biofeedback. 2014;39(3-4):171-180.
48. Motley HL. The effects of slow deep breathing on the blood gas exchange in emphysema. American Review of Respiratory Disease. 1963;88(4):484-492. 49. Berkenbosch A, Van Beek J, Olievier NC, De Goede J, Quanjer PH. Central respiratory CO2 sensitivity at extreme hypocapnia. Respiration physiology. 1984;55(1):95-102.
50. Malow BA, Edwards J, Marzec M, Sagher O, Fromes G. Effects of vagus nerve stimulation on respiration during sleep A pilot study. Neurology.
2000;55(10):1450-1454.
51. Mohan M, Saravanane C, Surange SG, Thombre DP, Chakrabarty AS. Effect of yoga type breathing on heart rate and cardiac axis of normal subjects. Indian J Physiol Pharmacol. 1986;30(4):334-340.
52. Mitchell RA, Berger AJ. Neural regulation of respiration. American Review of Respiratory Disease. 1975;111(2):206-224.
53. Shannon R. Intercostal and abdominal muscle afferent influence on medullary dorsal respiratory group neurons. Respiration physiology. 1980;39(1):73-94. 54. Merrill EG. The lateral respiratory neurones of the medulla: their associations with nucleus ambiguus, nucleus retroambigualis, the spinal accessory nucleus and the spinal cord. Brain research. 1970;24(1):11-28.
55. Plum F, Alvord EC. Apneustic breathing in man. Archives of neurology. 1964;10(1):101-112.
56. Biancardi V, Bícego KC, Almeida MC, Gargaglioni LH. Locus coeruleus noradrenergic neurons and CO2 drive to breathing. Pflügers Archiv-European Journal of Physiology. 2008;455(6):1119-1128.
57. Powley TL. Vagal input to the enteric nervous system. Gut. 2000;47(suppl 4):iv30-iv32.
58. Tewfik TL, Meyers AD. Vagus nerve anatomy. 2014.
59. Guyenet PG. The sympathetic control of blood pressure. Nature reviews. Neuroscience. 2006;7(5):335.
60. Bronzwaer A-SGT, Ouweneel DM, Stok WJ, Westerhof BE, van Lieshout JJ. Arterial Pressure Variation as a Biomarker of Preload Dependency in Spontaneously Breathing Subjects–A Proof of Principle. PloS one. 2015;10(9):e0137364.
61. Price K, Schartz P, Watson AHD. The effect of standing and sitting postures on breathing in brass players. SpringerPlus. 2014;3(1):210.
62. Haffor ASA. Effects of O2 Breathing on cardiac mitochondrial, Got, and free radical production. J. Med. Sci. 2004;4(2):164-169.
63. Pieczenik SR, Neustadt J. Mitochondrial dysfunction and molecular pathways of disease. Experimental and molecular pathology. 2007;83(1):84-92. 64. Nishikawa T, Edelstein D, Du XL, Yamagishi S-i. Normalizing mitochondrial superoxide production blocks three pathways of hyperglycaemic damage. Nature. 2000;404(6779):787.
65. Sena LA, Chandel NS. Physiological roles of mitochondrial reactive oxygen species. Molecular cell. 2012;48(2):158-167.
66. Hillman CH, Erickson KI, Kramer AF. Be smart, exercise your heart: exercise effects on brain and cognition. Nature reviews. Neuroscience. 2008;9(1):58. 67. Brown RP, Gerbarg PL. Sudarshan Kriya yogic breathing in the treatment of stress, anxiety, and depression: part I—neurophysiologic model. Journal of Alternative & Complementary Medicine. 2005;11(1):189-201.
68. Wager TD, Waugh CE, Lindquist M, Noll DC, Fredrickson BL, Taylor SF. Brain mediators of cardiovascular responses to social threat: part I: Reciprocal dorsal and ventral sub-regions of the medial prefrontal cortex and heart-rate reactivity. Neuroimage. 2009;47(3):821-835.
69. Fagard RH. Exercise characteristics and the blood pressure response to dynamic physical training. Medicine and science in sports and exercise. 2001;33(6 Suppl):S484-492; discussion S493-484.
70. Kurl S, Laukkanen JA, Rauramaa R, Lakka TA, Sivenius J, Salonen JT. Systolic blood pressure response to exercise stress test and risk of stroke. Stroke. 2001;32(9):2036-2041.
71. De Petrillo LA, Kaufman KA, Glass CR, Arnkoff DB. Mindfulness for long-distance runners: An open trial using Mindful Sport Performance Enhancement (MSPE). Journal of Clinical Sport Psychology.
2009;3(4):357-376.
72. Sydorchuk LP, Tryniak MH. Effect of voluntary regulation of the respiration on the functional state of the autonomic nervous system. Likars' ka sprava. 2004(1-2):65-68.
73. Takahashi T, Murata T, Hamada T, et al. Changes in EEG and autonomic nervous activity during meditation and their association with personality traits. International Journal of Psychophysiology. 2005;55(2):199-207.
74. Gourine AV, Kasymov V, Marina N, et al. Astrocytes control breathing through pH-dependent release of ATP. Science. 2010;329(5991):571-575. 75. Asahara T, Murohara T, Sullivan A, et al. Isolation of putative progenitor endothelial cells for angiogenesis. Science. 1997;275(5302):964-966. 76. Prior BM, Yang HT, Terjung RL. What makes vessels grow with exercise training? Journal of Applied Physiology. 2004;97(3):1119-1128.
77. Burri PH. Lung development and pulmonary angiogenesis. Lung development: Springer; 1999:122-151.
78. Wallin BG, Fagius J. Peripheral sympathetic neural activity in conscious humans. Annual review of physiology. 1988;50(1):565-576.
79. Borovikova LV, Ivanova S, Zhang M, et al. Vagus nerve stimulation attenuates the systemic inflammatory response to endotoxin. Nature.
2000;405(6785):458-462.
80. Cournand A, Motley HL, Werko L, Richards DW. Physiological studies of the effects of intermittent positive pressure breathing on cardiac output in man. American Journal of Physiology--Legacy Content. 1947;152(1):162-174.
81. Guyton AC. The relationship of cardiac output and arterial pressure control. Circulation. 1981;64(6):1079-1088.
82. Potter EK, McCloskey DI. Respiratory stimulatiion by angiotensin II. Respiration physiology. 1979;36(3):367-373.
83. Lumbers ER, McCloskey DI, Potter EK. Inhibition by angiotensin II of baroreceptor‐evoked activity in cardiac vagal efferent nerves in the dog. The Journal of Physiology. 1979;294(1):69-80.
84. Bach KB, Mitchell GS. Hypoxia-induced long-term facilitation of respiratory activity is serotonin dependent. Respiration physiology.
1996;104(2-3):251-260.
85. Cunningham DJC, Hey EN, Lloyd BB. The effect of intravenous infusion of noradrenaline on the respiratory response to carbon dioxide in man. Experimental Physiology. 1958;43(4):394-399.
86. Katz A, Liberty IF, Porath A, Ovsyshcher I, Prystowsky EN. A simple bedside test of 1-minute heart rate variability during deep breathing as a prognostic index after myocardial infarction. American heart journal. 1999;138(1):32-38.
87. Brasher PA, McClelland KH, Denehy L, Story I. Does removal of deep breathing exercises from a physiotherapy program including pre-operative education and early mobilisation after cardiac surgery alter patient outcomes? Australian Journal of Physiotherapy. 2003;49(3):165-173.